Pharmacotherapeutic group: Drugs for obstructive airways diseases, Adrenergics in combination with anticholinergics including triple combinations with corticosteroids.
ATC code: R03AL08.
PHARMACOLOGY: Pharmacodynamics: Mechanism of action: Fluticasone furoate, umeclidinium and vilanterol represent three classes of medications: a synthetic corticosteroid, a long-acting muscarinic receptor antagonist (also referred to as a LAMA or as an anticholinergic) and a selective, long-acting beta
2-receptor agonist (LABA), respectively.
Fluticasone furoate: Fluticasone furoate is a corticosteroid with potent anti-inflammatory activity. Corticosteroids have been shown to have a wide range of actions on multiple cell types (e.g. eosinophils, macrophages, lymphocytes) and mediators (e.g. cytokines and chemokines) involved in inflammation.
Umeclidinium: Umeclidinium is a long-acting pan-muscarinic receptor antagonist (also referred to as an anticholinergic). Umeclidinium exerts its bronchodilatory activity by competitively inhibiting the binding of acetylcholine with muscarinic cholinergic receptors on airway smooth muscle. It demonstrates slow reversibility at the human M3 muscarinic receptor subtype
in vitro and a long duration of action
in vivo when administered directly to the lungs in pre-clinical models.
Vilanterol: Vilanterol is a selective LABA. The pharmacologic effects of beta
2-adrenoceptor agonist drugs, including vilanterol, are at least in part attributable to stimulation of intracellular adenylate cyclase, the enzyme that catalyzes the conversion of adenosine triphosphate (ATP) to cyclic-3',5'-adenosine monophosphate (cyclic AMP). Increased cyclic AMP levels cause relaxation of bronchial smooth muscle and inhibition of release of mediators of immediate hypersensitivity from cells, especially from mast cells.
Pharmacodynamic effects: Cardiovascular effects: The effect of Trelegy Ellipta on the QT interval has not been evaluated in a thorough QT (TQT) study. TQT studies for fluticasone furoate/vilanterol and umeclidinium/vilanterol did not show clinically relevant effects on QT interval at clinical doses of fluticasone furoate, umeclidinium and vilanterol (see as follows).
The effect of umeclidinium/vilanterol on the QT interval was evaluated in a placebo and moxifloxacin controlled QT study involving once daily administration of umeclidinium/vilanterol 125/25 micrograms or 500/100 micrograms for 10 days in 103 healthy volunteers. The maximum mean difference in prolongations of QT interval (corrected using the Fridericia method, QTcF) from placebo after baseline-correction was 4.3 (90% CI: 2.2, 6.4) milliseconds seen 10 minutes after administration with umeclidinium/vilanterol 125/25 micrograms and 8.2 (90% CI: 6.2, 10.2) milliseconds 30 minutes after administration with umeclidinium/vilanterol 500/100 micrograms. No clinically relevant effect on prolongation of QT interval (corrected using the Fridericia method) was observed at the umeclidinium/vilanterol 125/25 micrograms dose. In addition, no clinically significant effects of umeclidinium/vilanterol on cardiac rhythm were observed on 24-hour Holter monitoring in 281 patients who received umeclidinium/vilanterol 125/25 micrograms once daily for up to 12 months.
The effect of fluticasone furoate/vilanterol on the QT interval was evaluated in a double-blind, multiple-dose, placebo- and positive-controlled crossover study in 85 healthy volunteers. The maximum mean (95% upper confidence bound) difference in QTcF from placebo after baseline-correction was 4.9 (7.5) milliseconds and 9.6 (12.2) milliseconds seen 30 minutes after dosing with fluticasone furoate/vilanterol 200/25 micrograms and fluticasone furoate/vilanterol 800/100 micrograms, respectively. A dose-dependent increase in heart rate was also observed. The maximum mean (95% upper confidence bound) difference in heart rate from placebo after baseline-correction was 7.8 (9.4) beats/min and 17.1 (18.7) beats/min seen 10 minutes after dosing with fluticasone furoate/vilanterol 200/25 micrograms and fluticasone furoate/vilanterol 800/100 micrograms, respectively.
No clinically relevant effects on the QTc interval were observed on review of centrally read ECGs from 911 subjects with COPD exposed to Trelegy Ellipta for up to 24 weeks, or in the subset of 210 subjects exposed for up to 52 weeks.
Clinical Studies: Study 1: The efficacy of Trelegy Ellipta (FF/UMEC/VI 100/62.5/25 micrograms) administered as a once daily treatment in patients with a clinical diagnosis of COPD has been evaluated in one 24-week active-controlled study with an extension up to 52 weeks in a subset of patients (study CTT116853, FULFIL).
All patients were required to have a smoking history of at least 10 pack years; a post-salbutamol FEV
1/FVC ratio <0.70; a clinical diagnosis of COPD, and a post-bronchodilator FEV
1 of <50% predicted normal or a post-bronchodilator FEV
1 <80% predicted normal and a history of ≥2 moderate exacerbations or one severe (hospitalised) exacerbation in the previous 12 months at screening. At screening, the mean post-bronchodilator FEV
1 was 45.5% predicted, and the mean reversibility was 8.17%. Approximately 55% of patients had a history of ≥2 moderate or ≥1 severe COPD exacerbations in the 12 months prior to screening.
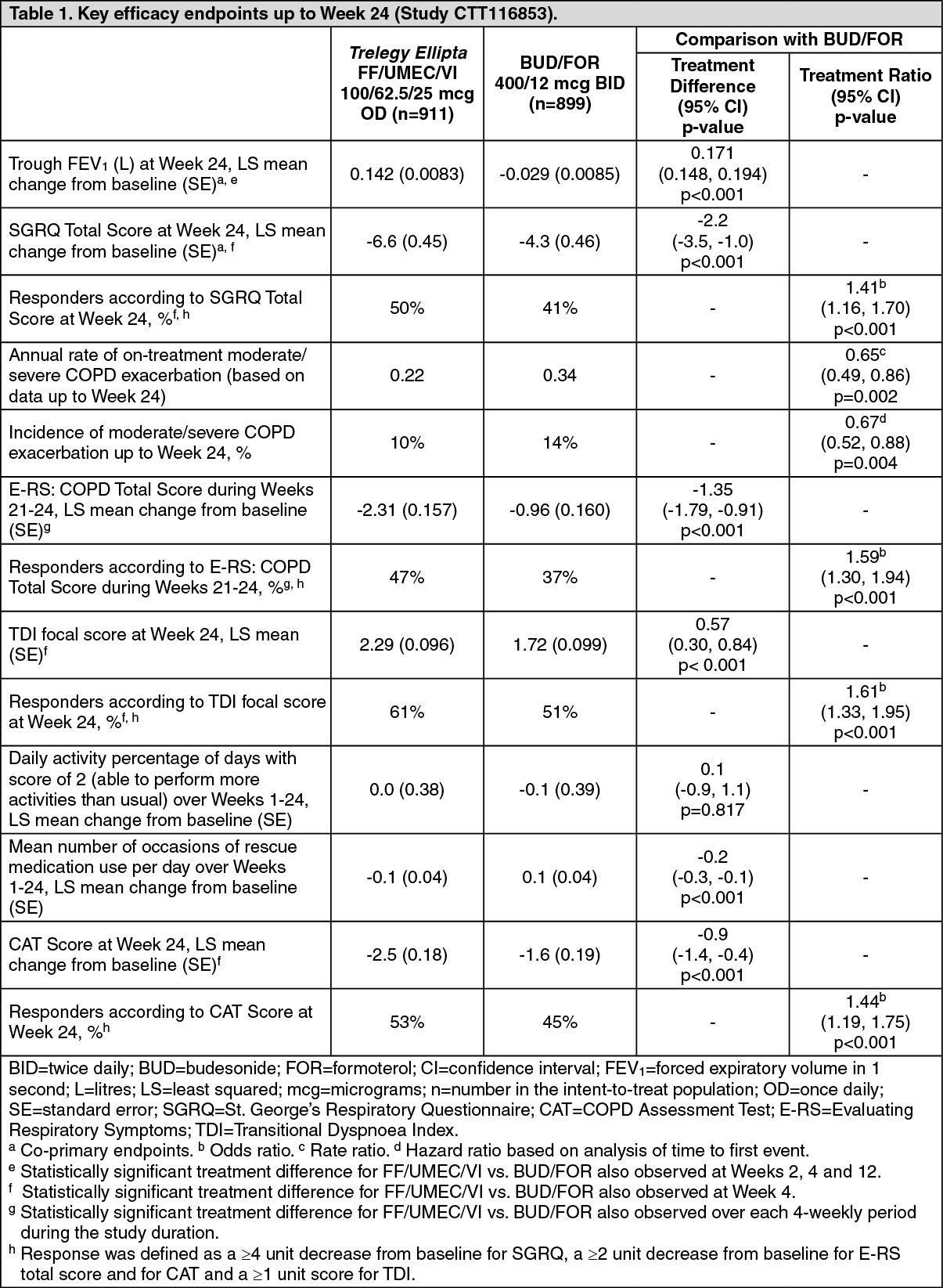
Trelegy Ellipta 100/62.5/25 micrograms administered once daily demonstrated a statistically significant improvement in lung function (as defined by change from baseline trough FEV
1 at Week 24; co-primary endpoint) compared with budesonide/formoterol (BUD/FOR) 400/12 micrograms administered twice-daily (see Table 1). Bronchodilatory effects with Trelegy Ellipta were evident on the first day of treatment and were maintained over the 24-week treatment period.
Trelegy Ellipta demonstrated a statistically significant improvement compared with BUD/FOR at Week 24 for Health Related Quality of Life (HRQoL) measured by the St. George's Respiratory Questionnaire (SGRQ) total score (co-primary endpoint), SGRQ responder analysis, COPD Assessment Test (CAT) score and CAT responder analysis, and also for respiratory symptoms measured using the Evaluating Respiratory Symptoms in COPD (E-RS: COPD) score and sub-scale scores over Weeks 21-24, breathlessness measured using the Transitional Dyspnoea Index (TDI) focal score at Week 24, and rescue medication use measured by mean number of occasions per day over Weeks 1-24 (see Table 1).
Trelegy Ellipta demonstrated a statistically significant reduction in the annual rate of moderate/severe exacerbations (i.e. requiring treatment with antibiotics or corticosteroids or hospitalisation; extrapolated from data up to Week 24) compared with BUD/FOR. A reduction in the risk of a moderate/severe exacerbation was observed with Trelegy Ellipta compared with BUD/FOR (based on analysis of the time to first exacerbation) (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The lung function, HRQoL, symptoms and exacerbations outcomes up to 52 weeks of treatment in a subset of patients (n = 430) were consistent with the results up to 24 weeks.
Study 2: The long-term efficacy of Trelegy Ellipta (FF/UMEC/VI 100/62.5/25 micrograms) administered once daily in patients with COPD with a history of moderate or severe exacerbations within the prior 12 months has been evaluated in a 52-week, active-controlled study compared with the fixed-dose combination of fluticasone furoate/vilanterol (FF/VI 100/25 micrograms) and umeclidinium/vilanterol (UMEC/VI 62.5/25 micrograms) (randomization 2:2:1) (study CTT116855, IMPACT).
Patients treated with Trelegy Ellipta demonstrated a statistically significant reduction in the annual rate of on-treatment moderate/severe exacerbations (primary endpoint) compared with FF/VI and compared with UMEC/VI. See Table 2 for efficacy endpoint results. (See Table 2.)
Click on icon to see table/diagram/image
The effects on lung function (change from baseline trough FEV
1) of Trelegy Ellipta compared with FF/VI and UMEC/VI for trough FEV
1 were observed at all timepoints over the course of the 52-week study (see figure).
Click on icon to see table/diagram/image
The reduction in the mean number of occasions/day of beta
2-agonist rescue medication use and the percentage of 24-hour periods without need of rescue medication was statistically significant in patients receiving Trelegy Ellipta compared with FF/VI or UMEC/VI at Weeks 49 to 52 (see Table 3) and these differences were observed over the course of the 52-week study.
Patients receiving Trelegy Ellipta had statistically significantly greater reduction in nighttime awakenings due to COPD symptoms compared with FF/VI or UMEC/VI at Weeks 49 to 52 (see Table 3) and these differences were observed over the course of the 52-week study for UMEC/VI and for the majority of timepoints for FF/VI. (See Table 3.)
Click on icon to see table/diagram/image
Treatment with Trelegy Ellipta demonstrated a clinically meaningful improvement of -2.0 points for COPD Assessment Test (CAT) score change from baseline at Week 52. Differences were statistically significant when compared with FF/VI (-0.5; 95% CI: -0.8, -0.2; p<0.001) and with UMEC/VI (-0.4; 95% CI: -0.8, -0.1; p=0.021).
The CAT responder rate (defined as 2 units below baseline or lower) at Week 52 was statistically significantly higher for patients treated with Trelegy Ellipta (42%) compared with FF/VI (37%; odds ratio 1.24; 95% CI: 1.14, 1.36; p<0.001) and with UMEC/VI (36%; odds ratio 1.28; 95% CI: 1.15, 1.43; p<0.001).
Breathlessness, measured using the Transitional Dyspnoea Index (TDI) focal score at Week 52, was measured in a subset of patients (N = 5,058 from 10 countries: Belgium, Canada, Czech Republic, Denmark, Germany, Netherlands, Poland, Spain, UK, USA). Treatment with Trelegy Ellipta (n = 2,029) demonstrated a statistically significant improvement compared with FF/VI (n = 2,014), LS mean TDI focal score of 0.98 and 0.71, respectively, a difference of 0.27 (95% CI: 0.04, 0.49; p=0.020). A statistically significant effect was not observed between Trelegy Ellipta and UMEC/VI (n = 1,015), LS mean TDI focal score of 0.98 and 0.89, respectively, a difference of 0.09 (95% CI: - 0.19, 0.37; p=0.522). The proportion of responders by TDI (defined as at least 1 unit) was statistically significantly higher for Trelegy Ellipta (36%) compared with FF/VI (29%; odds ratio 1.36; 95% CI: 1.19, 1.55; p<0.001) and UMEC/VI (30%; odds ratio 1.33; 95% CI: 1.13, 1.57; p<0.001) at Week 52.
Other supporting efficacy studies: Study 200812 was a 24-week, non-inferiority study (N = 1,055) that compared Trelegy Ellipta (FF/UMEC/VI 100/62.5/25 micrograms), administered as a single inhaler, with fluticasone furoate/vilanterol (100/25 micrograms) + umeclidinium (62.5 micrograms), co-administered as multi-inhaler therapy, once daily to patients with a history of moderate or severe exacerbations within the prior 12 months. In this study, FF/UMEC/VI was noninferior compared with FF/VI + UMEC in the improvement from baseline in trough FEV
1 at week 24. The pre-specified non-inferiority margin was 50 mL.
Umeclidinium with fluticasone furoate/vilanterol: In two 12-week, placebo controlled studies (200109 and 200110), the addition of umeclidinium (62.5 micrograms) to fluticasone furoate/vilanterol (FF/VI) (100/25 micrograms) once daily in adult patients with a clinical diagnosis of COPD, resulted in statistically significant and clinically meaningful improvements in the primary endpoint of trough FEV1 at Day 85 compared with placebo plus FF/VI (124 mL [95% CI: 93, 154; p<0.001] in study 200109 and 122 mL [95% CI: 91, 152; p<0.001] in study 200110).
12-month studies with fluticasone furoate/vilanterol: Two 52-week randomised, double-blind, parallel-group studies (HZC102970 and HZC102871) compared the annual rate of moderate/severe exacerbations in adult patients with a clinical diagnosis of COPD, treated with FF/VI or with vilanterol once daily. The results of an integrated analysis of both studies showed that treatment with FF/VI 100/25 micrograms once daily resulted in a 27% reduction in the annual rate of moderate/severe COPD exacerbations compared with vilanterol (95% CI: 16, 37; p<0.001). Reductions in risk of moderate/severe exacerbation (based on analysis of time to first exacerbation) and rate of exacerbations requiring corticosteroid use were also observed with FF/VI 100/25 micrograms once daily compared with vilanterol.
Pharmacokinetics: When fluticasone furoate, umeclidinium, and vilanterol were administered in combination by the inhaled route from a single inhaler in healthy subjects, the pharmacokinetics of each component were similar to those observed when each active substance was administered either as fluticasone furoate/vilanterol combination, umeclidinium/vilanterol combination, or each component as monotherapy.
Population PK analyses for fluticasone furoate/umeclidinium/vilanterol were conducted using a combined PK dataset from three phase III studies in 821 COPD subjects. Systemic drug levels (steady-state C
max and AUC) of fluticasone furoate, umeclidinium and vilanterol following fluticasone furoate/umeclidinium/vilanterol in one inhaler (triple combination) were within the range of those observed following fluticasone furoate/vilanterol plus umeclidinium administered via two inhalers, dual combinations (fluticasone furoate/vilanterol and umeclidinium/vilanterol), as well as individual single inhalers (fluticasone furoate, umeclidinium, and vilanterol).
Absorption: Fluticasone furoate: Following inhaled administration of Trelegy Ellipta in healthy subjects, fluticasone furoate C
max occurred at 15 minutes. The absolute bioavailability of fluticasone furoate when administrated as fluticasone furoate/vilanterol by inhalation was on average 15.2%, primarily due to absorption of the inhaled portion of the dose delivered to the lung, with negligible contribution from oral absorption. Following repeat dosing of inhaled fluticasone furoate/vilanterol, steady state was achieved within 6 days with up to 1.6-fold accumulation.
Umeclidinium: Following inhaled administration of Trelegy Ellipta in healthy subjects, umeclidinium C
max occurred at 5 minutes. The absolute bioavailability of inhaled umeclidinium was on average 13%, with negligible contribution from oral absorption. Following repeat dosing of inhaled umeclidinium, steady state was achieved within 7 to 10 days with 1.5 to 2-fold accumulation.
Vilanterol: Following inhaled administration of Trelegy Ellipta in healthy subjects, vilanterol C
max occurred at 7 minutes. The absolute bioavailability of inhaled vilanterol was on average 27%, with negligible contribution from oral absorption. Following repeat dosing of inhaled fluticasone furoate/vilanterol, steady state was achieved within 6 days with up to 1.5-fold accumulation.
Distribution: Fluticasone furoate: Following intravenous administration of fluticasone furoate to healthy subjects, the mean volume of distribution was 661 litres.
In vitro plasma protein binding in human plasma was >99.6%.
Umeclidinium: Following intravenous administration of umeclidinium to healthy subjects, the mean volume of distribution was 86 litres.
In vitro plasma protein binding in human plasma was on average 89%.
Vilanterol: Following intravenous administration of vilanterol to healthy volunteers, the mean volume of distribution at steady state was 165 litres.
In vitro plasma protein binding in human plasma was on average 94%.
Metabolism: Fluticasone furoate:
In vitro studies showed that fluticasone furoate is metabolised principally by CYP3A4 and is a substrate for the P-glycoprotein (P-gp) transporter. Fluticasone furoate is primarily metabolised through hydrolysis of the S-fluoromethyl carbothioate group to metabolites with significantly reduced corticosteroid activity. Systemic exposure to the metabolites is low.
Umeclidinium:
In vitro studies showed that umeclidinium is metabolised principally by CYP2D6 and is a substrate for the P-gp transporter. The primary metabolic routes for umeclidinium are oxidative (hydroxylation, O-dealkylation) followed by conjugation (glucuronidation, etc), resulting in a range of metabolites with either reduced pharmacological activity or for which the pharmacological activity has not been established. Systemic exposure to the metabolites is low.
Vilanterol:
In vitro studies showed that vilanterol is metabolised principally via CYP3A4 and is a substrate for the P-gp transporter. The primary metabolic routes are O-dealkylation to a range of metabolites with significantly reduced beta
1- and beta
2-agonist activity. Plasma metabolic profiles following oral administration of vilanterol in a human radiolabel study were consistent with high first-pass metabolism. Systemic exposure to the metabolites is low.
Drug-drug interactions: A repeat dose study was performed in healthy subjects with the fluticasone furoate/vilanterol combination (200/25 micrograms) and ketoconazole (400 milligrams, a strong CYP3A4 inhibitor and Pgp inhibitor). Co-administration increased mean fluticasone furoate AUC
(0-24) and C
max by 36% and 33%, respectively. The increase in fluticasone furoate exposure was associated with a 27% reduction in 0-24 hours weighted mean serum cortisol. Co-administration increased mean vilanterol AUC
(0-t) and C
max by 65% and 22%, respectively. The increase in vilanterol exposure was not associated with an increase in beta-agonist related systemic effects on heart rate or blood potassium.
Fluticasone furoate, umeclidinium and vilanterol are substrates of P-gp. A repeat dose drug interaction study performed in healthy subjects who were administered with umeclidinium/vilanterol or umeclidinium, and the P-gp and moderate CYP3A4 inhibitor verapamil (240 milligrams), did not show any clinically significant effect on the pharmacokinetics of vilanterol or umeclidinium.
The effect of a CYP2D6 poor metaboliser genotype on the steady-state pharmacokinetics of umeclidinium was assessed in healthy volunteers (CYP2D6 normal metabolisers and CYP2D6 poor metabolisers). No clinically meaningful difference in systemic exposure to umeclidinium (500 micrograms which is eight-fold higher than the therapeutic dose) was observed following repeat daily inhaled dosing to normal and CYP2D6 poor metaboliser subjects.
Elimination: Fluticasone furoate: The apparent plasma elimination half-life of fluticasone furoate following inhaled administration of fluticasone furoate/vilanterol was, on average, 24 hours. Following intravenous administration, the elimination phase half-life averaged 15.1 hours. Plasma clearance following intravenous administration was 65.4 litres/hour. Urinary excretion accounted for approximately 2% of the intravenously administered dose. Following oral administration, fluticasone furoate was eliminated in humans mainly by metabolism with metabolites being excreted almost exclusively in faeces, with <1% of the recovered radioactive dose eliminated in the urine.
Umeclidinium: Umeclidinium plasma elimination half-life following inhaled dosing for 10 days averaged 19 hours, with 3% to 4% drug excreted unchanged in urine at steady-state. Plasma clearance following intravenous administration was 151 litres/hour. Following intravenous administration, approximately 58% of the administered radiolabelled dose was excreted in faeces and approximately 22% of the administered radiolabelled dose was excreted in urine. The excretion of the drug-related material in the faeces following intravenous dosing indicated secretion into the bile. Following oral administration, 92% of the administered radiolabelled dose was excreted primarily in faeces. Less than 1% of the orally administered dose (1% of recovered radioactivity) was excreted in urine, suggesting negligible absorption following oral administration.
Vilanterol: Vilanterol plasma elimination half-life following inhaled dosing for 10 days averaged 11 hours. Plasma clearance of vilanterol following intravenous administration was 108 litres/hour. Following oral administration of radiolabelled vilanterol, 70% of the radiolabel was excreted in urine and 30% in faeces. Primary elimination of vilanterol was by metabolism followed by excretion of metabolites in urine and faeces.
Special Patient Populations: In a population pharmacokinetic analysis (n = 821), the impact of demographic covariates (race/ethnicity, age, gender, weight) on the pharmacokinetics of fluticasone furoate, umeclidinium, and vilanterol was evaluated. Renal and hepatic impairment were assessed in separate studies.
Race: In East Asian subjects with COPD (Japanese and East Asian Heritage) (n = 113) who received fluticasone furoate/umeclidinium/vilanterol, estimates of fluticasone furoate AUC
ss were on average 30% higher compared with Caucasian subjects. However, these higher systemic exposures are not expected to have a clinically relevant effect on 24 hour serum or urinary cortisol excretion. There was no effect of race on pharmacokinetics of umeclidinium or vilanterol in subjects with COPD.
No clinically relevant differences requiring dose adjustment based on race were observed in fluticasone furoate, umeclidinium or vilanterol systemic exposure.
Elderly: No clinically relevant effects requiring dose adjustment based on age were observed.
Renal impairment: Trelegy Ellipta has not been evaluated in subjects with renal impairment. However, studies have been conducted with fluticasone furoate/vilanterol and umeclidinium/vilanterol.
A clinical pharmacology study of fluticasone furoate/vilanterol showed that severe renal impairment (creatinine clearance <30 mL/min) did not result in significantly greater exposure to fluticasone furoate or vilanterol or more marked corticosteroid or beta
2-agonist systemic effects compared with healthy subjects.
A study in subjects with severe renal impairment administered with umeclidinium/vilanterol showed no evidence of an increase in systemic exposure to either umeclidinium or vilanterol (C
max and AUC).
In vitro protein binding studies between subjects with severe renal impairment and healthy volunteers were conducted, and no clinically significant evidence of altered protein binding was seen.
The effects of haemodialysis have not been studied.
Hepatic Impairment: Trelegy Ellipta has not been evaluated in subjects with hepatic impairment. However, studies have been conducted with fluticasone furoate/vilanterol and umeclidinium/vilanterol.
Following repeat dosing of fluticasone furoate/vilanterol for 7 days, there was an increase in fluticasone furoate systemic exposure (up to three-fold as measured by AUC
(0-24)) in subjects with hepatic impairment (Child-Pugh A, B or C) compared with healthy subjects. The increase in fluticasone furoate systemic exposure (fluticasone furoate/vilanterol 200/25 micrograms) in subjects with moderate hepatic impairment (Child-Pugh B) was associated with an average 34% reduction in serum cortisol compared with healthy subjects. In subjects with severe hepatic impairment (Child-Pugh C) that received fluticasone furoate/vilanterol 100/12.5 micrograms there was no reduction in serum cortisol (10% increase in serum cortisol).
Following repeat dosing of fluticasone furoate/vilanterol for 7 days, there was no significant increase in systemic exposure to vilanterol (C
max and AUC) in subjects with mild, moderate, or severe hepatic impairment (Child-Pugh A, B or C).
There were no clinically relevant effects of the fluticasone furoate/vilanterol combination on beta-adrenergic systemic effects (heart rate or serum potassium) in subjects with mild or moderate hepatic impairment (vilanterol, 25 micrograms) or with severe hepatic impairment (vilanterol, 12.5 micrograms) compared with healthy subjects.
Subjects with moderate hepatic impairment showed no evidence of an increase in systemic exposure to either umeclidinium or vilanterol (C
max and AUC), and no evidence of altered protein binding by umeclidinium or decreased protein binding by vilanterol between subjects with moderate hepatic impairment and healthy volunteers was observed
in vitro.
Umeclidinium has not been evaluated in subjects with severe hepatic impairment.
Other patient characteristics: No clinically relevant differences requiring dose adjustment based on the effect of gender, weight or body mass index were observed.
CYP2D6 poor metabolisers showed no evidence of a clinically significant effect of CYP2D6 genetic polymorphism on systemic exposure to umeclidinium.
Toxicology: Preclinical Safety Data: Pharmacological and toxicological effects seen with fluticasone furoate, umeclidinium or vilanterol in nonclinical studies were those typically associated with glucocorticoids, muscarinic receptor antagonists, or beta
2-adrenergic receptor agonists. Administration of combined fluticasone furoate, umeclidinium and vilanterol to dogs did not result in any significant new toxicity or any major exacerbation of expected findings associated with fluticasone furoate, umeclidinium or vilanterol alone.
Carcinogenesis/mutagenesis: Fluticasone furoate was not genotoxic in a standard battery of studies and was not carcinogenic in lifetime inhalation studies in rats or mice at AUC exposures 1.4- or 2.9-fold, respectively, those in humans given fluticasone furoate 100 micrograms.
Umeclidinium was not genotoxic in a standard battery of studies and was not carcinogenic in lifetime inhalation studies in mice or rats at exposures ≥ 20- or ≥ 17-fold the human clinical exposure at umeclidinium 62.5 micrograms, based on AUC, respectively.
Genetic toxicity studies indicate vilanterol does not represent a genotoxic hazard to humans. Consistent with findings for other beta
2-agonists, in lifetime inhalation studies vilanterol caused proliferative effects in the female rat and mouse reproductive tract and rat pituitary gland. There was no increase in tumour incidence in rats or mice at exposures 0.9- or 22-fold, respectively, the human clinical exposure of vilanterol at 25 micrograms based on AUC.
Reproductive Toxicology: Neither fluticasone furoate nor umeclidinium nor vilanterol had any adverse effects on male or female fertility in rats.
Fluticasone furoate was not teratogenic in rats or rabbits, but delayed development in rats and caused abortion in rabbits at maternally toxic inhaled doses. There were no effects on development in rats at exposures 6.6-fold the human clinical exposure at 100 micrograms, based on AUC. Fluticasone furoate had no adverse effect on pre- or post-natal development in rats.
Umeclidinium was not teratogenic in rats or rabbits. In a pre- and post-natal study, subcutaneous administration of umeclidinium to rats resulted in lower maternal body weight gain and food consumption and slightly decreased pre-weaning pup body weights in dams given 180 micrograms/kg/day dose (approximately 61-fold the human clinical exposure at 62.5 micrograms umeclidinium, based on AUC).
Vilanterol was not teratogenic in rats. In inhalation studies in rabbits, vilanterol caused effects similar to those seen with other beta
2-agonists (cleft palate, open eyelids, sternebral fusion and limb flexure/malrotation). When given subcutaneously there were no effects at exposures 62-fold the human clinical exposure at 25 micrograms, based on AUC. Vilanterol had no adverse effect on pre- or post-natal development in rats.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image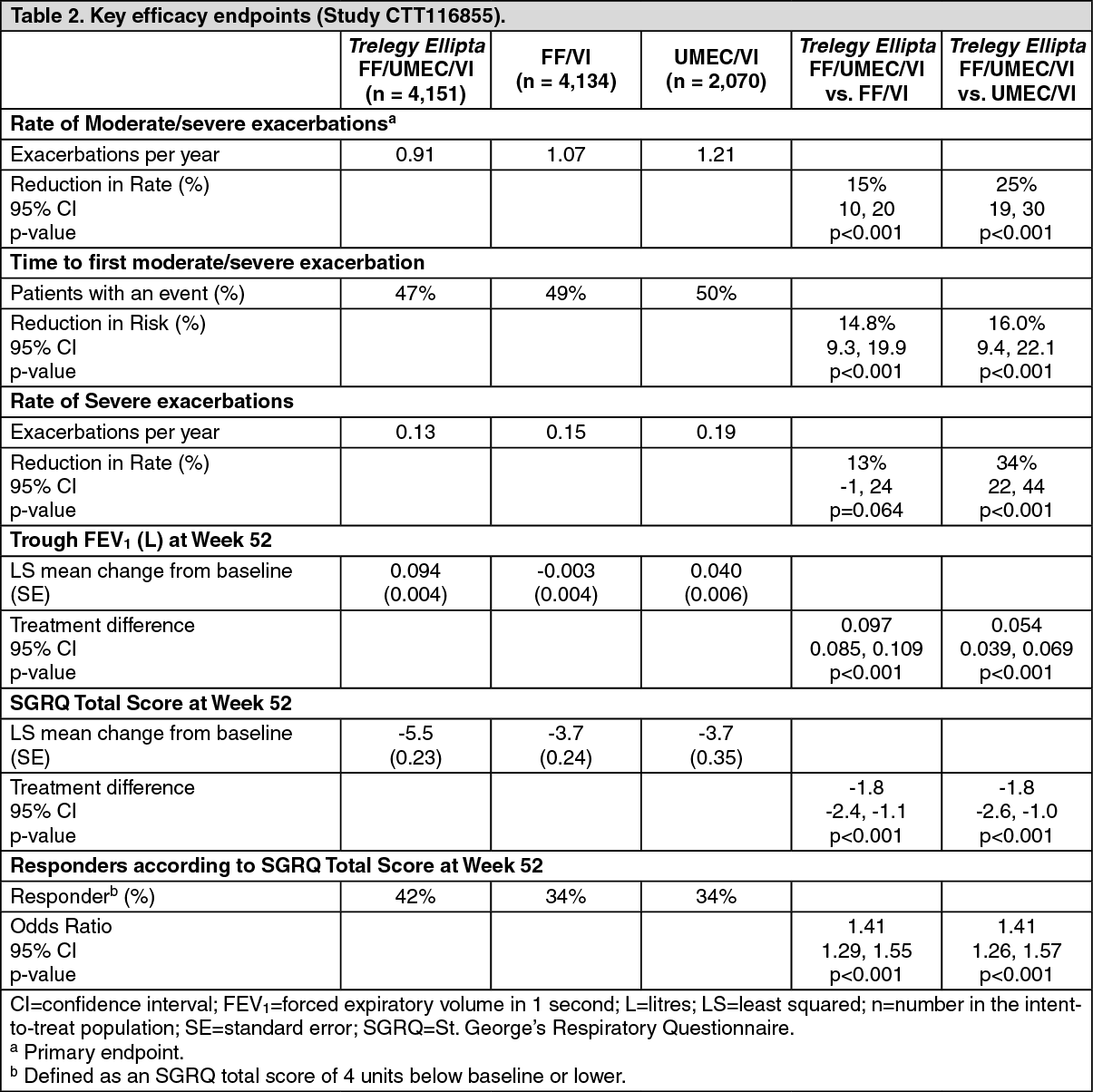 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image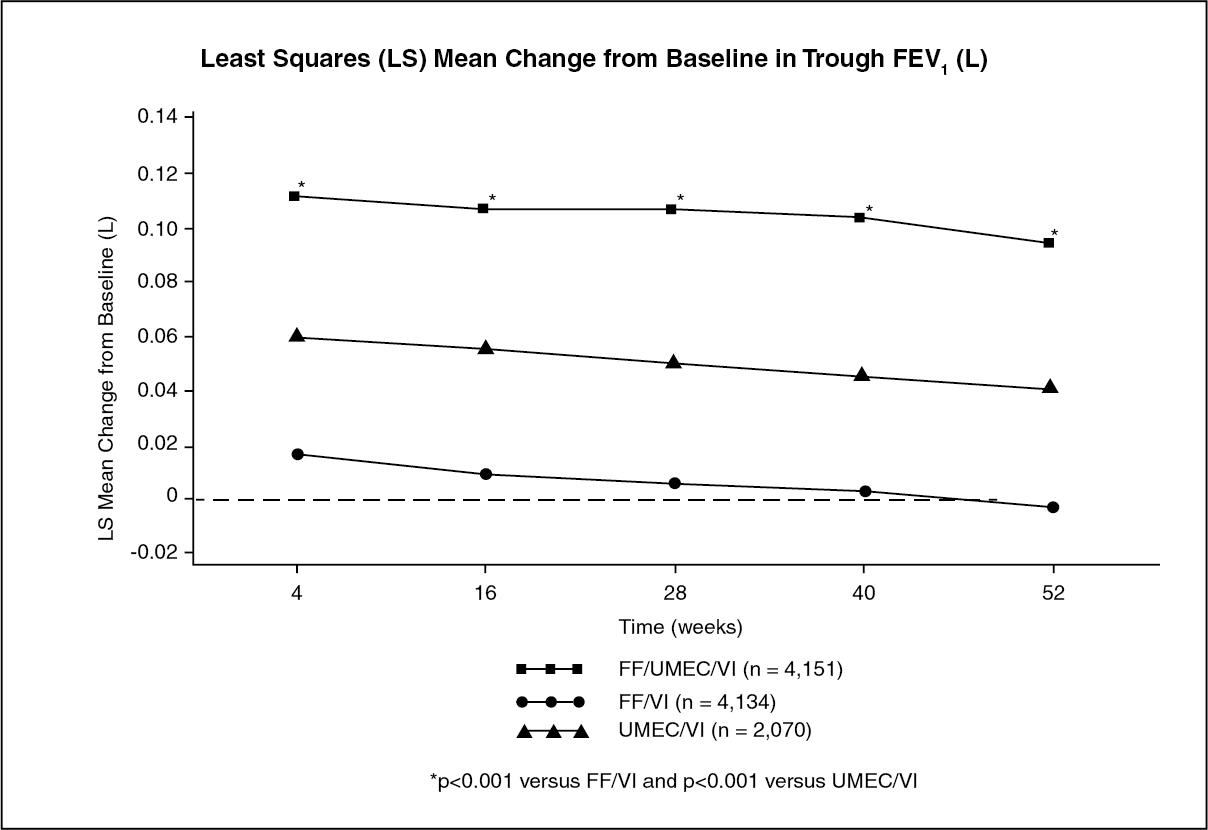 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image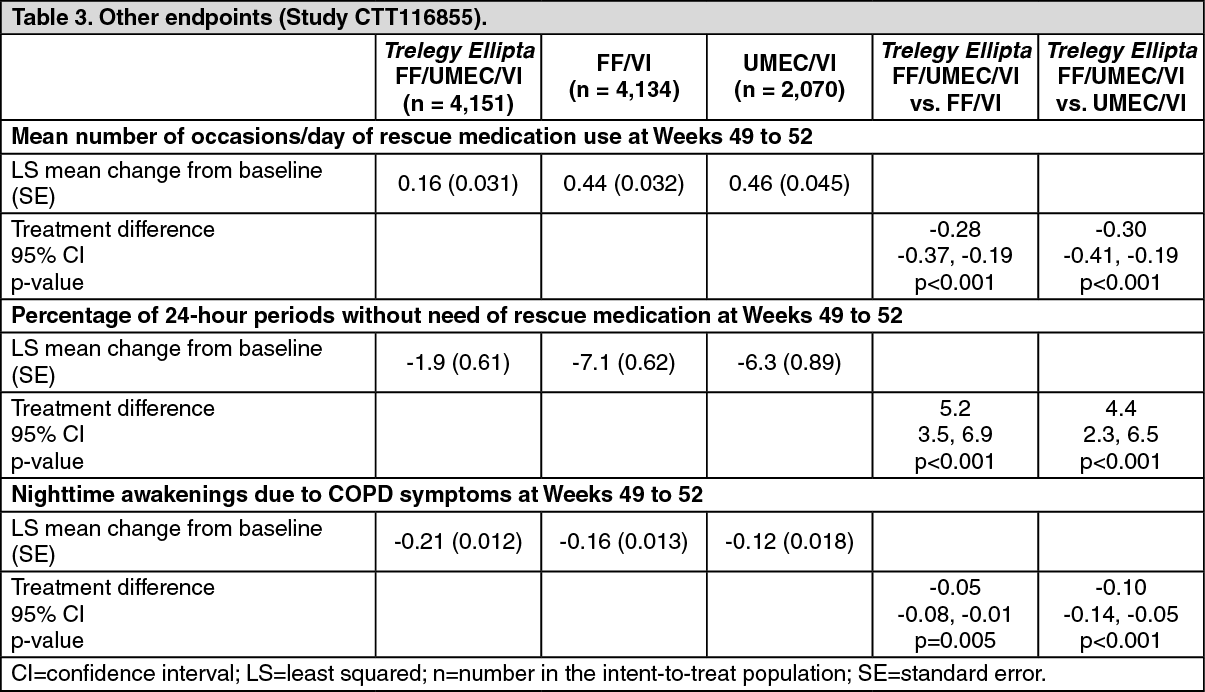 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
